

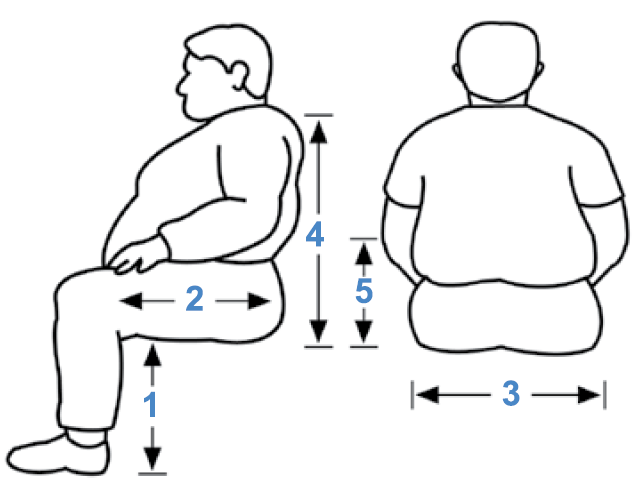
- Seat distance from floor (Seat Height)
- Depth of seat from front to rear (Seat Depth)
- Overall width of seat (Seat Width)
- Seat to top of back (Back Rest Height)
- Seat to top of armrest (Armrest Height)
- Back Angle (degrees)
If the seat plane is not parallel to the floor. Indicate the distance from the front and rear of seat to floor. - Front Edge to Floor
- Rear Edge to Floor
Please check for environmental access restrictions.Tell us the maximum overall width, wheel to wheel, to ensure passage through doorways, ramps, etc.
Gendron recommends that specifications to build each wheelchair be supplied by a physician, physical therapist or other qualified medical professional.
Actual Body Weight.
If client body type is pear-like, consider potential of stable weight and stable wheelchair width over time. If client body type is apple-like, consider potential for fluctuating weight. If deciding between two sizes, consider opting for larger size and potentially wider wheelchair.
Custom Measuring for the Wheelchair User.
If possible, have the client sit on a hard surface such as a therapy mat or a square of firm plywood. The client’s thighs should be level and not upward or downward sloping relative to the hip joint. The lower leg should be in a natural, vertically oriented posture. This posture allows for easy access to measure the client from a true postural set, otherwise not possible from a soft surface. Once the overall height is determined, the next consideration in wheelchair measurement is the pelvis, as this is the primary weight-bearing surface.
- Seat Height: With feet flat on the floor and the shin in a vertical posture, measure from the back of the heel to the underside of the knee. The client should wear their typical footwear, and again the thighs should be level relative to the hip joint prior to measurement. This will allow for proper foot rest length and overall wheelchair height which is so vital in wheelchair propulsion, as the obese population tend to achieve propulsion by a combination of hand and foot use.
Wheelchair floor to seat height is also critical for sit to stand activities. For individuals who are primarily exercise ambulators, a lower seat height may be indicated allowing community propulsion, while individuals who ambulate to vital rooms or bathrooms, a higher seat height may be indicated. Recall that wheelchair cushions will add to the height of the finished sitting surface. - Seat Depth: Measure from the back of the buttocks to within 2 inches of the back of the knee. The completed wheelchair should allow for approximately 2 inches of space between the back of the client’s knee and the front of the wheelchair seat, thereby preserving circulation to the lower leg while maximizing the client’s weight-bearing surface and leg mobility during foot-assisted propulsion. The seat surface should support the entire gluteal region.
- Seat Width: Measure widest part of the client in seated posture. Again consider apple versus pear. A pear-shaped individual having greater gluteal femoral weight distribution may be widest near the front edge of the seat. Excessive wheelchair width will restrict mobility about environmental barriers, increase difficulty of turning and decrease arm support with resulting potential for back pain. The completed wheelchair will allow for approximately 1 to 2 inches of width on either side of the client for winter clothing, client weight shifting during pressure relief and, if necessary, room for possible lift devices such as slings. On occasion, clients may opt to remove wheelchair push rims to accommodate narrow barriers.
- Back Rest Height: Measure from the seat surface to mid-shoulder-blade height. The back rest generally should reach to mid-shoulder-blade level in height and support the apex of the client’s back to diminish potential for postural back pain and provide for adequate pressure relief while allowing maximal shoulder-blade mobility. If the client is in a reclining chair then additional upper thoracic support may be indicated. More agile clients may prefer a back rest that is positioned vertically just 1 inch below the shoulder blade, allowing for maximal upper body mobility over their lower trunk in sitting postures. If a client may have localized excessive tissue bulk causing partial contact to their back rest, a strap or laced back rest may be necessary to provide sufficient support for that unique body type.
- Armrest Height: Measure directly from the sitting surface to the bent elbow having the forearm parallel to the seat. Recall that a seat cushion may add to the height of the seat and equally add to the height of the armrest. Appropriate armrest height is determined from this measurement and is important for decreasing neck and thoracic back pain by providing adequate support for the shoulder girdle. Remember that respiratory-impaired individuals derive increased respiratory support by leaning upon their forearms and thereby increase depth of breathing by reverse action of upperbody muscles. This is common in the obese client with respiratory compromise of congestive heart failure.
*Measuring Guidelines reprinted with permission of Michael Dionne, PT, Choice Physical Therapy, Inc.